
Dr Connon has trained with leading surgeons in Australia, France, the UK and US to employ techniques to perform patients’ knee replacements in a way that optimises pain relief, function and minimises recovery duration.
Dr Connon was one of the pioneer surgeons performing the quadriceps-sparing (subvastus) approach to knee replacement surgery on the Sunshine Coast and hasn’t looked back since, having performed many hundreds of knee replacements using this technique in the last few years. This technique can offer a faster reduction in pain and recovery of range of motion according to the combined results of multiple research trials (A meta-analysis of randomised controlled trials – the highest standard of medical research). The end outcomes are the same as a ‘conventional’ (medial parapatellar) approach, which is still the most common way to perform a total knee replacement in Australia.
If you have you have severe knee pain that has stopped responding to less-invasive treatments such as tablets and physiotherapy, you may benefit from knee replacement. This can help reduce your pain and improve your mobility to get you back to doing the things you love. Total or partial knee replacement works by surgically removing part or all of a worn and painful joint and replacing it with a man-made joint (known as a prosthesis). Most people can return to normal life within 3 months of a knee replacement and you can return to many activities sooner.
There are different ways of performing a knee replacement and we can help you choose the right technique for your circumstances.
Total knee replacement is the most common type of knee replacement (about 90% of knee replacements in Australia) and involves replacing all of the arthritic knee joint surfaces on the femur (thigh bone), tibia (shin bone) and patella (kneecap). The advantage of replacing all of these surfaces at once is it reduces the chance of you ever requiring further surgery on that knee.
We can talk to you further about the numerous techniques that have been developed in recent years to ensure you have a smoother recovery from your knee replacement. Knee replacements also last longer than previously due to improved techniques and materials.
If you have advanced knee arthritis with severe pain and/or compromise of your quality of life despite trying non-operative measures, you may benefit from a total knee replacement. This is where the arthritis surfaces of your knee joint are removed and replaced with a ‘prosthetic knee’. Knee replacement surgery doesn’t have to be nearly as sore as it once was – thanks to a combination of advances in muscle/tendon/ligament preservation, kinematic alignment, better implants, anaesthetic techniques and postoperative pain minimisation with ice, elevation and less aggressive physiotherapy protocols. We will discuss these with you more in clinic in the pre-oeprative education session that all patients are invited to.
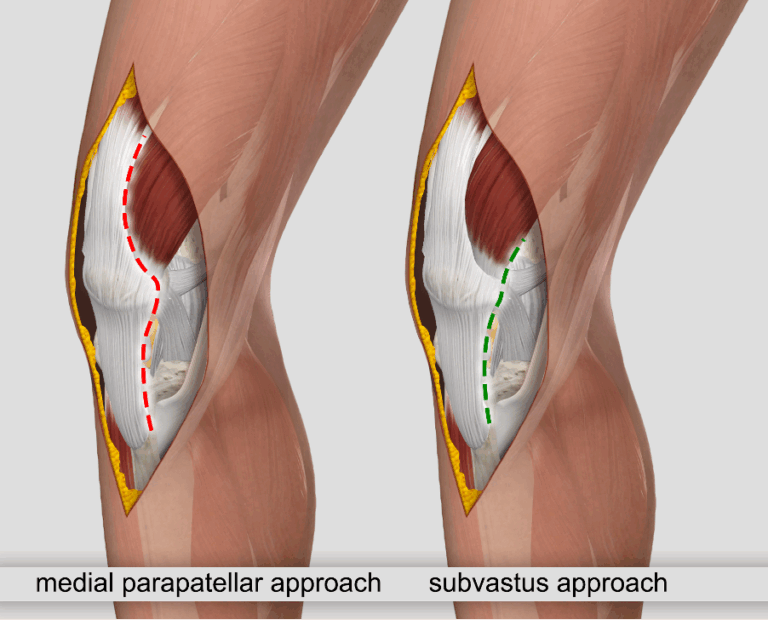
Dr Connon has been performing all his first-time (primary) total knee replacements using a quadriceps-sparing (‘subvastus’) approach since late 2023. and has performed more knee replacements using this technique than any other surgeon on the Sunshine Coast. This technique avoids cutting any muscle/tendon and is called the ‘sub-vastus’ approach because it goes ‘sub’ (underneath) the vastus medialis muscle, rather than cutting through the quadriceps tendon/extensor mechanism, which is how a ‘traditional’ medial parapatellar approach is executes as shown in this picture. For more information, please see Dr Connon’s recent blog post here.
Partial knee replacement can be the right option for patients with osteoarthritis that is limited to a small section of the knee (medial compartment primarily) with a particular interest in certain sporting activities (examples include tennis and surfing). If you have a knee that is only worn in this part, with minimal angulation of your leg, an intact ACL, and meet several other criteria, this may be the best option for you. Dr Connon will t
There are different ways to optimise the positioning of a knee replacement prosthesis and your surgeon can help advise which is best for your circumstances.

Robotic surgery involves the placement of several “tracking” pins in the thigh bone (“femur”) and shin bone (“tibia”) which are used to tell the computer where the knee is. A robotic arm then helps guide Dr Connon where to make the surgical cuts to implant the knee replacement in the desired position. The robot does not perform the cuts- it simply assists in guiding the surgeon where to make those cuts.
Dr Connon can talk to you about the best technique for performing your knee replacement surgery and whether robotically assisted knee replacement is right for you.
A CT scan and a standing Xray of your leg alignment is used to map out your anatomy and prepare a 3D printed model of your knee. After calculating the loss of the cartilage that has occurred from your arthritis, Dr Connon can then restore your alignment to what it was before the arthritis developed (“kinematic alignment”).
Your surgeon can then determine the appropriate size of knee replacement for your knee, and where they need to make their cuts to restore your pre-arthritic lower limb alignment whilst preserving your ligaments and giving you a knee that is both mobile and stable.
To ensure this plan is accurately executed in the operating theatre, patient specific instrumentation is then 3D-printed to sit accurately on your unique knee anatomy intraoperatively and guide where the necessary cuts are to be made.
Dr Connon can talk to you about the best technique for performing your knee replacement surgery and whether patient specific instrumentation is right for you.
Anaesthesia for knee replacement surgery usually involves spinal anaesthetic or general anaesthetic and many patients actually have some of each to optimise their pain relief and post-operative recovery. Dr Connon and your anaesthetist can discuss the most appropriate anaesthetic options for you.
To begin, Dr Connon will make an incision over the knee. He will then remove the damaged bone and cartilage from the knee joint.
The damaged arthritic surfaces are replaced with metal components covering the femur (thigh bone) and tibia (shin bone). A hard-wearing polyethylene (plastic) wafer is placed in between these two metal components to allow them to glide smoothly on each other. These are generally held in place with bone cement (polymethylmethacrylate). Finally, the arthritic surface of the patella (kneecap) is replaced with a polyethylene component.
The time spent in hospital following knee replacement surgery varies according to your needs and personal circumstances as a patient. To go home we need to ensure your pain is well controlled and you can safely get around your own home with the use of crutches or another gait aid to assist you as required. The majority of patients spend about 3-4 days in hospital, but some people are keen and suitable to go home earlier and some patients can stay for longer- it is dependent on your specific circumstances.
It is becoming relatively uncommon for patients to need inpatient rehabilitation after a total knee replacement because various advances in recent years have ensured most patients are able to recover faster with less pain from their surgery and are hence able to safely return directly to their own home. Community services have also significantly improved so many patients choose the comfort of their own home. Some patients still require inpatient rehabilitation, and this is usually determined based on how the individual progresses with physiotherapy after surgery- we can’t always predict it beforehand. We will do our best to tailor your post-operative rehabilitation program to your needs and preferences.
After your anaesthetic has worn off, you should be able to place full weight on your knee, with crutches or a frame to aid you. It is preferable that if your operation is done earlier in the day, you stand up on the same day as surgery to get used to being upright again. Sometimes you will even be able to go for a short walk.
We will try to get you walking, sometimes with a frame, sometimes with only crutches as an aid.
When you are comfortable and once you are able to walk independently and tackle stairs, that’s when you are safe to head home. Everybody is a little different and this timeframe is tailored to you as an individual.
After 2-3 weeks, your wound will be checked (usually by a specialist wound nurse). Dr Connon will normally use dissolving suture and glue, so no suture removal is likely to be required. After your wound review you should arrange to see your physiotherapist to begin post-operative exercises. We recommend against seeing your physio before the wound review to allow the wound to settle first.
By two weeks you are probably down to using a single crutch in the opposite hand to your knee replacement. You will use this for longer walks and balance but can actually often get short distances around home without a gait aid. You will gradually disband this remaining crutch over the next few weeks depending on your stability.
From 6 weeks post-surgery, you should be able to return to many normal activities though longer walks will probably still cause a bit of discomfort. Please note that the purpose of the 6 week review if to check you are on track: you will not yet be completely healed. You will certainly still have some swelling at this stage: it is normal to have swelling for months which settles gradually. Some patients may be able to drive earlier, notably following a left knee replacement if you have an automatic car.
Dr Connon will always put your health first and will discuss the potential risks of surgery with you before you book in for any procedure. Before surgery, Dr Connon will assess any risks involved with your current medications, medical history, and require your skin to be healthy. He will also organise a review by a perioperative doctor to optimise your general medical health and monitor you postoperatively.
Some risks present themselves only after surgery, such as infection and DVT. Please don’t hesitate to call Dr Connon’s rooms if you have any postoperative concerns.
You should be able to do many normal activities after 6 weeks though heavy manual labour and certain sports can take longer. Please note that time frames differ for each patient.
Physiotherapy is important to your recovery. Your priority is to maximise your range of movement, both bending and straightening your leg. After a week or two, you can slowly begin increasing your walking distance and building your strength and stability. Note that although the swelling starts to settle after 1-2 weeks it can persist for over 3 months so the use of ice and/or a compression bandage can aid with this and thus improve range of motion.

Advances in surgical techniques and prosthetics mean that you can expect knee replacement surgery to last for longer than previously. Many people still recall that older style prostheses would last “about 10 or 15 years” but this is because those older implants used plastics that wore away much faster.
Australian Joint Replacement Registry data shows that using modern implants, 80-90% of knee replacements last for 20 years or more. Most patients therefore only need their knee replacement done once.
Whilst the need for revision knee replacement (re-do surgery to replace a worn-out replacement) is much more likely in younger patients, there is no specific age-limit on knee replacement surgery.
From being admitted to hospital to returning to the ward, the entire process of knee replacement surgery will take several hours. This includes preparation for surgery and recovering (waking up) afterwards. The surgery itself usually takes approximately one hour when performed by an experienced surgeon but is dependent on how complex your anatomy is.
While every individual is different, and recovery can be affected by many factors, you should expect to resume normal life by 6-12 weeks after surgery depending on the specific task. For example, you should be able to walk everyday distances such as around the shops by 6 weeks, but not yet do heavy manual labour for example.
Most of the cost of your knee replacement will be covered by your health insurance. We can advise you of any remaining likely out-of-pocket costs for after your consultation which is dependent on which health fund you are with. These vary based on your fund and type of cover but will be itemised for you in detail after your pre-operative consultation. Dr Connon has arrangements with many health funds that limit your out-of-pocket costs.
Due to Dr Connon’s expertise in performing day surgery knee replacement, he is particularly experienced at treating patients seeking to “self-fund” their knee replacement. This is because one of the main costs of total knee replacement is the hospital stay and the total cost can therefore be lowered by shortening your hospital stay where it is safe to do so. Some patients are even able to go home on the day of surgery.
Rough total costs are generally around $21,000 – 25,000 depending on your length of stay. Please note that Dr Connon will never agree to lower the cost of your operation by using substandard implants or compromising on safety so some costs are unavoidable and corners will not be cut.
You are generally allowed to return to most activities of normal life after a knee replacement, even more strenuous ones such as skiing. Please be aware that higher impact use of your knee replacement may result in it wearing out sooner. Please also note that some patients report difficulty with kneeling down after knee replacement.